
COVID Has A Lower Mortality Risk To Children Than The Flu, Car Accidents, Suicide & More

The risks of severe illness and death from COVID for children has not been put in context of other risks. Right now, many parents are stricken with fear and worry about their child contracting COVID. Putting COVID in the context of other risks may help change the perspective of parents and also question whether or not making COVID vaccines mandatory for children is the right decision.
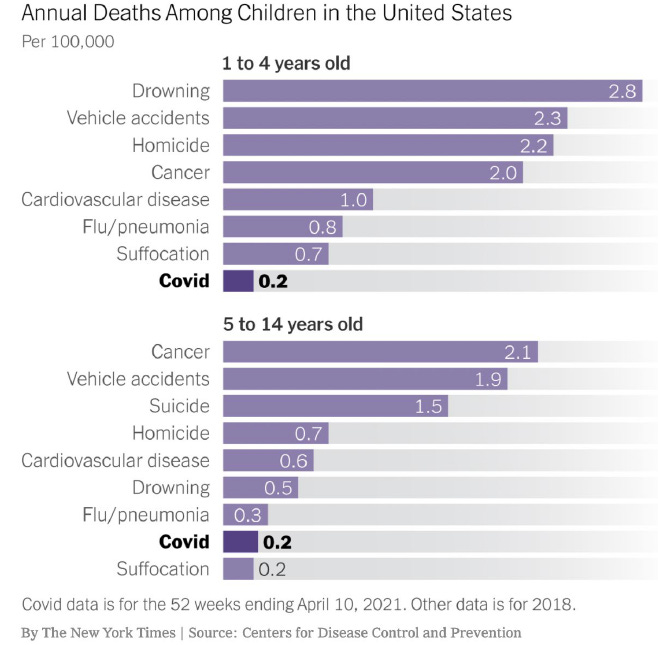
When it comes to morality risk to children, COVID-19 has a lower annual mortality risk than car accidents, influenza, and for 5-14 year olds, suicide (Leonhardt, 2021). In fact, the survival rate of COVID for people under the age of 19 according to recent pre-print study by two Stanford scientists is nearly 100 percent.
Seroprevalence data from eight locations around the world: England, France; Ireland; Netherlands; Spain; Atlands, USA; New York, USA; Geneva, Switzerland show the infection fatality rate for 0-9 year olds to be less than 1 in 200,000 (less than 5 in 1 million) and 1/55,000 for 10–19-year-olds.
Even the risk of hospitalization as a result of a COVID infection is quite low. If infected with COVID-19, children ages 0-9 have on average a chance of 0.1% or 1/1000 of being hospitalized and, for ages 11-19 a 0.2% or 1/500 chance of being admitted to the hospital
(Herrera-Esposito, 2021).
In Canada, as of May 28, 2021, there were 259,308 confirmed cases of SARS-CoV-2 infections in Canadians 19 years and under. Of these, 0.48% were hospitalized, 0.06% were admitted to ICU, and 0.004% died. According to this data, seasonal influenza is associated with more severe illness than COVID-19.
Given Canada's numbers, the discussion around "keeping children safe at school" is not a policy concern if it was not one for the seasonal flu. Yes, children may be a source of transmission, but they are not at risk of COVID by being at school.
While many studies suggest pre-symptomatic/asymptomatic spread may comprise > 40% of vertical transmission, numerous large observational population studies show that children are POOR COVID-19 spreaders. This includes studies from Ireland, Iceland, Italy, France, and Australia. For a link to a more complete reference list, see Washington University Pediatric & Adolescent Ambulatory Research Consortium.
In comparison to the vaccine, a study out of the University of California shows that the risk of myocarditis is greater after two doses of the Pfizer vaccine than being hospitalized for COVID for boys ages 12-15. The research was led by led by epidemiologist Dr. Tracy Høeg, an epidemiologist studying COVID in kids.
There have been multiple reports of death from myocarditis following COVID vaccination, including a 13-year-old Michigan boy who died June 16, three days after he received his second dose of Pfizer’s COVID vaccine. Preliminary autopsy results indicated that following his vaccination his heart become enlarged and was surrounded by fluid. As of August 7th, there were 106 reported incidents of myocarditis/pericarditis in Ontario, Canada in people under the age of 25.
Pfizer BioNTech study included 2,260 children and adolescents, 12-15 years of age, 1,131 of whom received the vaccine. This is a very small number of adolescents and does not permit an evaluation of rare but serious side-effects, such as effects that may happen in only 1:5,000 adolescents. Furthermore, with most of the adolescents followed for only 1 or 2 months after their 2nd dose, there is no data to support long-term safety.
Furthermore, the science regarding waning vaccine immunity and the science regarding natural immunity is something to consider as well, as well as the data showing that the vaccines offer a very low absolute risk reduction.
On the 22nd of September, Høeg gave her testimony to the U.S. House of Representatives providing an excellent summary regarding the latest data on COVID and kids. In it she cites data illustrating that drowning, vehicle accidents, homicide, cancer, cardiovascular disease, flu, and suffocation are all greater threats when it comes to mortality for children.
She also touches upon concerns like long COVID, and the Delta variant, and other affects the pandemic and health policy is having on the mental and physical health of children.
She outlines how the delta variant has resulted in increased case numbers in children, but the severity of the disease per case does not appear to have increased. When it comes to long COVID, a recent report from the Office of National Statistics (ONS, 2021) in the UK that she sites, the prevalence of persistent symptoms 12-16 weeks after COVID were no different between those with a COVID infection and controls.
I feel that our country’s failure to do a risk-benefit analysis as well as good scientific studies of the interventions we imposed upon children to mitigate one disease has created numerous additional and avoidable public health crises in our youth. For a disease that relatively spares them, this generation has suffered an incredible amount during the pandemic and, unfortunately, the effects of this will likely travel with them for the rest of their lives.
Høeg.
Sunetra Gupta, an infectious disease epidemiologist from the University of Oxford, Carl Heneghan, an NHS urgent care doctors and Professor of Evidence Based Medicine at the University of Oxford, as well as Alberto Giubilini, senior research fellow in infectious diseases at Oxford, make their position on vaccinating children quite clear below. They published an opinion article in the European Journal of Medical Ethics in July 2021, explaining why children should not be required or encouraged to take the COVID-19 vaccine.
The risks of COVID-19 for children and young people are minimal. For example, ‘[i]n the USA, UK, Italy, Germany, Spain, France and South Korea, deaths from COVID-19 in children remained rare up to February 2021 (ie, up to the time the study had available data about), at 0.17 per 100 000 population’.7 The long-term risks of the novel COVID-19 vaccines on a population of millions of children are at the moment unknown, given that the clinical trials involved a few thousands of subjects over a few months period.
Vaccinating children would be a way of treating them as mere means to serve other people’s interests or some form of collective good. We already did this through indiscriminate lockdowns and other restrictions, such as school closure. Using children as means or even mere means in this way is not necessarily wrong, but it can only be justified if the cost imposed is sufficiently small and the benefit sufficiently large.7 Unfortunately, currently available COVID-19 vaccines do not meet either condition, given our current state of knowledge. Not only would vaccinating children pose risks on them without any substantial direct benefit.
Also, vaccinating children can only offer collective good if this reduces infection levels in the community. However, while COVID-19 vaccines almost certainly will provide long-term protection against severe disease and death, their infection blocking effects are incomplete and very likely to be transient. This means there is actually no collective benefit to trade off against individual harm to children, unless we perform mass vaccination on a regular basis, for example, annually. But this would compound the potential harms.