
DTP & Five Other Vaccines Associated With Increased Overall Female Mortality
The whole-cell DTP vaccine used in low-income countries is associated with increased mortality for females. The observation has not been contradicted by good prospective studies.

Set Your Pulse: Take a breath. Turn your attention to your body and release any tension. Breathe slowly into the area of your heart for 60 seconds, focusing on feeling a sense of ease. Stay connected to your body as you read. Click here to learn why we suggest this.
Dr Christina Stabell Benn is a medical doctor (1996), PhD (2003) and Doctor of Medical Science (2011) from the University of Copenhagen. She is a Professor at the Odense Patient Data Explorative Network (OPEN) at the Faculty of Health Sciences at SDU and Professor in Global Health since 2013. She is considered a world-renowned vaccine expert.
Her research group, the Bandim Health Project (BHP), was established in 1978. It is not a government group. Apart from receiving some core funding from the Danish state and the University of Southern Denmark, they are primarily funded by grants for specific research projects. They apply for these grants from governmental and private foundations. The funders have no role in the studies. They an independent research group with no conflicts of interest.
She and her team have consistently found that the DTP vaccine is strongly associated with a higher risk of dying. This effect is more prominently seen in girls. Despite being protected against three deadly diseases, girls who received the DTP vaccine had a higher risk of dying than girls who did not receive it.
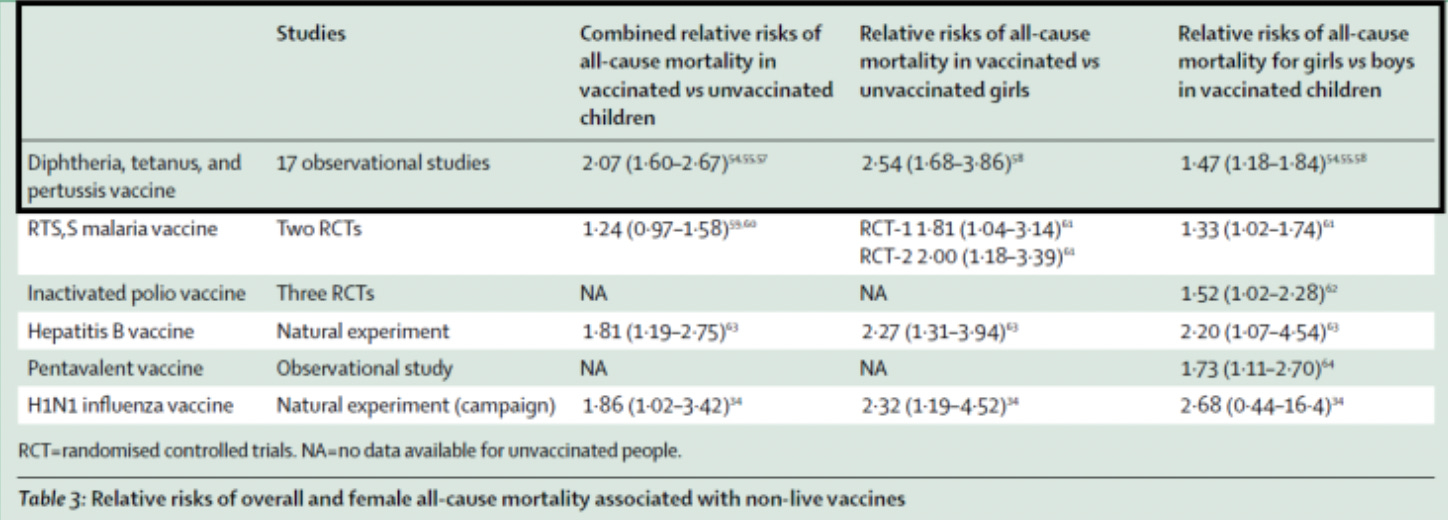
Her (and her team) work on this matter has shown that being DTP vaccinated vs. not being DTP vaccinated is associated with 2.07 (95% CI=1.60-2.67)-fold higher mortality. The estimate was 2.54 (1.68-3.86) in females. Among DTP-vaccinated children, females had almost 50% higher mortality than males (1.47 (1.18-1.84)). A dose-response has been observed, with the female-male mortality ratio increasing with each additional dose of DTP vaccine.
According to her, “The conclusion is very clear: The whole-cell DTP vaccine used in low-income countries is associated with increased mortality for females. The observation has not been contradicted by good prospective studies. What remains unclear is why WHO does not act.”
But the DTP vaccine is not the only vaccine that is associated with increased overall female mortality. The same pattern has been seen for six non-live vaccines. These include the RTS, S malaria vaccine, inactivated polio vaccine, Hepatitis B Vaccine, Pentavalent vaccine, and the H1N1 influenza vaccine.
Many of these observations have been reported in Guinea-Bissau, and the findings have been consistent in countries such as Benin, India, and Malawi.
It’s also important to mention that the opposite pattern is seen for live vaccines. They are associated with beneficial Non Specific Effects and decreased overall mortality, particularly for females. No bias can explain why only non-live vaccines should be negative for females. That being said, non live vaccines do have their fair share of criticisms and non-specific effects throughout medical literature as well. Like aluminum containing vaccines for example. You can read about those concerns here.
For clarity, live vaccines use a weakened (or attenuated) form of the germ that causes a disease. Non-live (inactivated) vaccines use killed pathogens, components of microbes, or mRNA to trigger an immune response.
“Vaccines have been shown in numerous randomized controlled trials, primarily in low-income settings, to have non-specific health effects. Live attenuated vaccines have been shown to harness beneficial non-specific effects (leading to reduced risk of non-target diseases or overall mortality). However, non-live vaccines have been observed to be associated with negative non-specific effects (increased risk of non-target infections and mortality, primarily in females). The effects are seen as long as a given vaccine is the most recent and can be reversed with a new type of vaccine. The current system for testing, approving and monitoring vaccines is not set up to capture non-specific effects and has serious limitations when it comes to capturing adverse events. Thus, studies of vaccines should aim to look at overall health impacts and not just the impact on the target disease. This is particularly important when the risk of the target disease is low.”
- Tracey Beth Høeg, Md, PhD and Dr Christine Stabell Benn in their piece,
When a vaccine is studied to prevent a specific illness, a study only examining how well that vaccine targets that illness is not enough. We must look for other things (non-specific effects), it’s obvious that a study is not going to find what it’s not looking for.
This news has been out a few years, since 2019?
Oh yeah, aluminum in vaccines? Are you effing kidding me? No wonder people are dying!!!! Give me a break!!!